Iron deficiency in childhood and adolescents

Iron is an essential element for the body and is involved in numerous physiological processes; it promotes the formation of hemoglobin and the maturation of red blood cells, supports the immune system and normal cognitive function. In younger people the lack of adequate iron intake during childhood can have negative effects on growth both in terms of physical and cognitive development.
Human body contains about 3-4 g total of iron, which is mostly recycled and distributed between the bloodstream and various organs. The amount that we introduce daily with food is very low, equal to about 1-2 mg and derives mainly from some foods such as: liver, offal, seafood, meat, fish, milk, some types of green vegetables (spinach), legumes (beans), dried fruit and cocoa.
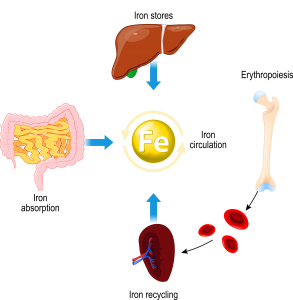
Figure 1: Iron metabolism in pur body.
Heme iron comes in the form of a ferrous ion (Fe2+) and is bound to particular proteins (globins) that favor its entry into the bloodstream and about 15-35% is absorbed by the intestine; heme iron represents 40% of the iron present in meat foods. Non-heme iron, on the other hand, can be found, according to its oxidation state, as a ferrous ion (Fe2+) or as a ferric ion (Fe3+) and constitutes 100% of vegetable foods. Ferrous iron is soluble and easily passes inside duodenal enterocytes, while ferric iron must be transformed into Fe2+ to be absorbed by the intestine. The percentage of absorption of non-heme iron is very low, about 5-12%.
Once it enters the bloodstream, iron circulates bound to a specific transport protein, called transferrin, which is carried throughout the body and it is partly stored in the form of ferritin mainly in the liver, spleen, bone marrow and, as well as, in myoglobin within muscle tissue.
Iron deficiency in childhood and adolescents
Children (2-12 years) are highly vulnerable and may experience iron deficiency (sideropenia) due to the rapid increase in blood volume and muscle mass during growth and development. Other factors that contribute to the increase in iron requirements are weight gain and physical activity. For this reason, the recommended iron intake in this period is about 7-9 mg per day.
Situations of iron deficiency can also appear during adolescence (12-18 years), a period characterized by a high need for iron due to rapid growth. Especially in young girls, with the onset of blood loss in the first menstrual cycles, an unbalanced iron levels may be found. The recommended levels of iron (12-14 mg per day) can only be achieved through proper food intake, such as meat, fish, and vegetables, which very often are not appreciated by adolescents.
Lack of iron has been shown to affect correct brain function and cognitive development. Therefore, in cases where nutrition is not sufficient to ensure a proper iron intake, it may be necessary to supplement it.
The most common symptoms related to iron deficiency are:
- Pallor;
- Weakness;
- Dizziness;
- Irritability;
- Difficulty concentrating.
Hemoglobin values in children and adolescents
In children and adolescents, the amount of iron in the blood is mainly related to two factors: age and sex. Among the most relevant hematological parameters we find hemoglobin, a protein most present in the blood and contains iron inside. The following table shows the average and minimum values, divided by age and gender:
| Age | Average Hemoglobin value (g/dL) | Minimum Hemoglobin value (g/dL) |
| From 2 to 6 years | 12,5 | 11,5 |
| From 6 to 12 years | 13,5 | 11,5 |
| Females from 12 to 18 years | 14 | 12 |
| Males from 12 to 18 years | 14,5 | 13 |
A low level of hemoglobin in the blood can be caused by an unbalanced diet or by an increased demand for iron during growth. Iron is also essential for the baby to strengthen the immune system. When hemoglobin turns out to be below the minimum value, it is called iron deficiency anemia, and on the advice of the doctor or pediatrician it must be treated.
The World Health Organization (WHO) has found that anemia is widespread globally, affecting children and women of reproductive age. Anemia is associated with poor cognitive and motor development. Iron deficiency is considered the most common cause of anemia.
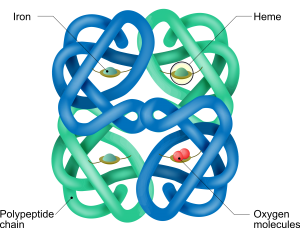
Figure 2: Hemoglobin structure.
Other markers in iron deficiency
Iron values in the body are measured by blood analysis of specific proteins that regulate its transport and storage:
- Sideremia, which measures the amount of circulating iron bound to transferrin;
- Transferrinemia, which measures the amount of transferrin, protein that transports iron to the organs and tissues;
- Saturation of transferrin, which indicates the percentage of saturated transferrin, i.e. that is binding iron compared to the total. The optimal values are between 20% and 50%;
- Ferritinemia, which measures the amount of ferritin, protein responsible for iron storage in the liver, muscles, and bone marrow.
Food supplements
Situations of iron deficiency can be recovered by eating iron-rich foods and, where this is not possible or insufficient, supplementing the normal diet with the intake of specific iron-based food supplements.
There are many iron-based foods dietary on the market, but not all of them contain the same source of iron, and the absorption of these occurs in the duodenum and proximal jejunum and depends heavily on the oxidation state of the iron. Iron is often characterized by a metallic aftertaste in the mouth and, once in contact with the gastric mucosa, can give irritative effects characterized by burning, nausea and constipation.
SiderAL® products contain Sucrosomial® Iron, in which ferric pyrophosphate (Fe3+) is transported within a matrix of phospholipids and sucrose esters of fatty acids.
Conclusion
The innovation of Sucrosomial® Technology is characterized by an excellent tolerability and it allows the iron intake anytime in the day (with meal or far from meals), for long periods of time, and prevents any discomfort commonly associated with iron intake, such as metallic and unpleasant aftertaste, irritation of the gastric mucosa, nausea or constipation. Overcoming the limits related to the conventional supplementation of iron, Sucrosomial® Iron promotes the intake of this important nutrient in all situations of deficiency or increased needs for iron.
BIBLIOGRAPHY
- WHO – World Health Organisation
- Sideral.it
- Craig W.J., Nutrition concerns and health effects of vegetarian diets., Nutr. Clin. Pract. 2010; 25: 613-20
- Hunt J.R., Bioavailability of iron, zinc, and other trace minerals from vegetarian diets., Am. J. Clin. Nutr. 2003; 78: 633S-9S
- Hurrell R., Egli I., Iron bioavailability and dietary reference values., Am. J. Clin. Nutr. 2010; 91: 1461S-7S
- Zimmermann M.B., Hurrell R.F., Nutritional iron deficiency., Lancet 2007; 370: 511-20
- Craig W.J., Iron status of vegetarians., Am. J. Clin. Nutr. 1994; 59: 1233S-7S
anemia Carenza di ferro integratori minerali salute sucrosomiale